Optimal Dextrose Concentration for Pain Control in Healthy Newborns during Hepatitis B Vaccination
Article information
Abstract
Purpose
Glucose has been recommended as an analgesic for mild to moderately painful procedures in neonates. The goal of this study was to assess the optimal dextrose concentration for pain control in newborns.
Methods
This prospective, randomized, blinded clinical trial included 116 healthy full-term newborns. The neonates were randomly assigned to the following four groups by drawing straws: groups receiving sterile water or a 10%, 20%, or 40% dextrose solution orally. Each group was treated with the assigned solution prior to hepatitis B vaccination. The Neonatal Facial Coding System (NFCS) and the Neonatal Infant Pain Scale (NIPS) scores were evaluated before, immediately after, and 2 minutes after the injection in all neonates. Premature Infant Pain Profile (PIPP) scores were evaluated during the injection. All procedures were video-recorded, and pain scores were assessed by two independent observers who were not involved in the care of the newborns studied. The pain scores were compared among the four groups.
Results
The 40% dextrose solution significantly reduced the NFCS (P=0.002) and the PIPP scores (P=0.001) compared with sterile water. No hyperglycemic events were noted in the study subjects 2 hours after the injection.
Conclusion
The 40% dextrose solution effectively relieved pain due to intramuscular injection in full-term newborns without causing hyperglycemic events. However, the 10% and 20% dextrose solutions did not affect neonatal pain scores.
INTRODUCTION
Repeated exposure to pain during infancy has been reported to be related to adverse neurodevelopmental outcomes that have both immediate and long-term effects [1-3]. Thus, the American Academy of Pediatrics and the Canadian Pediatric Society suggested the routine assessment of pain, minimizing the number of painful procedures, and managing pain using both pharmacologic and non-pharmacologic methods [4,5]. Witt et al. [6] also recommended the use of tiered anesthesia during painful procedures. The use of sweet solutions such as sucrose or glucose were recommended for mild to moderately painful procedures, as a sweet solution with non-nutritive sucking, skin-to-skin contact, and breastfeeding have reported synergistic effects [7-9].
The use of a 24% sucrose solution is usually recommended for neonatal pain control, although the exact oral dose has not been determined [10]. A recent meta-analysis of 38 studies reported that a 20% to 30% glucose solution was also effective against pain [11]. However, only a few studies included in this meta-analysis compared different glucose concentrations, and pain scores were not systematically analyzed.
This study aimed to assess the optimal concentration of dextrose for providing pain control in newborns. We evaluated the Neonatal Facial Coding System (NFCS) [12], Neonatal Infant Pain Scale (NIPS) [13], and Premature Infant Pain Profile (PIPP) [14] scores after the oral administration of sterile water or a 10%, 20%, or 40% dextrose solution prior to hepatitis B vaccination.
MATERIALS AND METHODS
This prospective, randomized, controlled, blinded clinical trial was conducted in the nursery of Gangneung Asan Hospital of Korea between January and October 2013. Written informed consent was provided by the parents of each subject prior to enrollment and the study was approved by the hospital’s Institutional Review Board (GNAH IRB No. 2013-044).
1. Subjects and randomization
Full-term newborn infants born at ≥37 weeks’ gestation with a birth weight ≥2,500 g were eligible to participate. Newborns with 1- or 5-minute Apgar scores <7 or those who needed close monitoring including pulse oximetry or repeated serum glucose levels were excluded. The newborns were randomly allocated, by drawing straws, to receive sterile water or 10%, 20%, or 40% dextrose prior to the administration of the vaccine.
2. Intervention
Each participant was orally administered 1 mL of sterile water or 10%, 20%, or 40% dextrose solution. Each solution was administered dropwise on the anterior part of the tongue with a 5-mL syringe to prevent any effect from sucking action. Two minutes later, the hepatitis B vaccine was administered to the thigh as an intramuscular injection of 0.5 mL using a 25-gauge needle (Euvax®, LG Life Sciences Ltd., Seoul, Korea). All procedures were performed when the newborns remained stable after more than 3 hours after birth to rule out the effect of birth-related conditions. We used no other non-pharmacologic analgesic methods such as non-nutritive sucking or skin-to-skin contact.
3. Pain monitoring and assessment
All interventions and physical appearance of newborns including facial expression and movement were video-recorded from the time of administration of the oral solution to 2 minutes after vaccination. Heart rates and oxygen saturation were monitored by a pulse oximeter placed on the left foot and video-recorded simultaneously. Two researchers who did not participate in the procedures, assessed pain scores separately, by analyzing the video recordings. The degree of pain was evaluated using the NFCS, NIPS, and PIPP scales in all groups. The NFCS and NIPS scores were assessed three times: before the injection (baseline), immediately after the injection (injection), and 2 minutes after the injection (recovery). We analyzed change in scores from baseline to injection and from baseline to recovery. The PIPP score was checked once during the injection. We calculated the mean of the scores assessed by the two researchers. The serum glucose level was checked at 2 hours after administration of the vaccine to assess hyperglycemia (defined as a serum glucose level >200 mg/dL).
4. Statistical analysis
Statistical analysis was performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). The changes in the NFCS and NIPS scores with different dextrose solutions were evaluated from baseline to injection and from baseline to recovery by repeated measures multivariate analysis of variance. The interaction between dextrose concentration and the onset time and the main effect of the dextrose concentration were evaluated. PIPP scores were evaluated by analysis of variance, while post hoc analysis was conducted by Bonferroni correction. P-values <0.05 were considered significant, while those <0.016 were subjected to Bonferroni correction.
RESULTS
A total of 120 newborns were enrolled and randomly assigned to four groups of 30 each. However, errors with video-recording occurred at three subjects in the sterile water group and one in the 10% dextrose group. Therefore, pain scores in 116 newborns were included in the final analysis: 27 in the sterile water group, 29 in the 10% dextrose group, 30 in the 20% dextrose group, and 30 in the 40% dextrose group.
The mean gestational age was 38.9±6.9 weeks and the mean birth weight, 3,212.9±342.6 g. The procedures were performed at a mean of 230.3±57.2 minutes after birth and 84.3±54.5 minutes after the most recent feed. There was no significant difference in clinical characteristics between the groups except the mode of delivery (Table 1). There was no difference in the mean serum glucose level checked 2 hours after injection among groups, and no hyperglycemic events were observed.
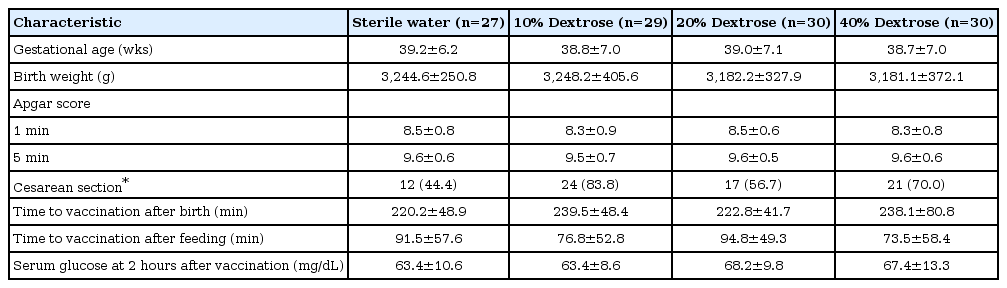
Characteristics of the Newborns
Tables 2, 3 present the mean NFCS, NIPS, and PIPP scores assessed by the two observers at each time point during the procedure, with different dextrose concentrations. Interobserver reliability showed good agreement; the intraclass correlations (ICC) were ≥0.8 for NFCS scores at recovery, NIPS scores at baseline and recovery, and PIPP scores compared to ≥0.6 for the other parameters.
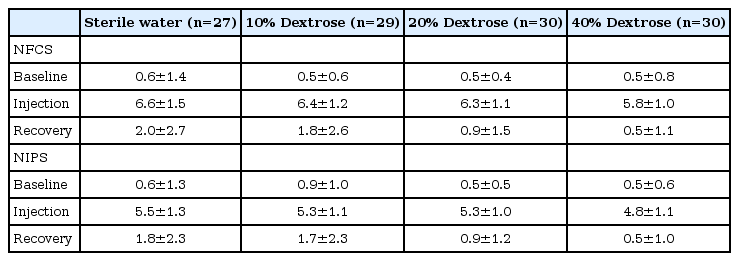
NFCS and NIPS Scores at Baseline, Injection, and Recovery
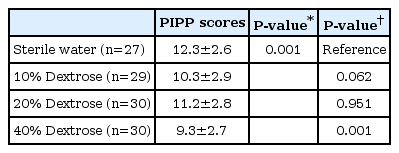
Comparison of PIPP scores
We compared the changes in NFCS and NIPS scores from baseline to injection and those from baseline to recovery between groups. The trend in change of scores were similar between groups in both NFCS (P=0.284) and NIPS (P=0.166). The 40% dextrose group showed significantly lower NFCS scores compared to the sterile water group regardless of the time of evaluation (P=0.002), while there was no difference in the change of NIPS scores between groups. The 10% and 20% dextrose groups showed no differences compared to the sterile water group on either pain scale (Table 4). Furthermore, PIPP scores showed a significant difference only between the sterile water and the 40% dextrose groups (P=0.001) (Table 3).
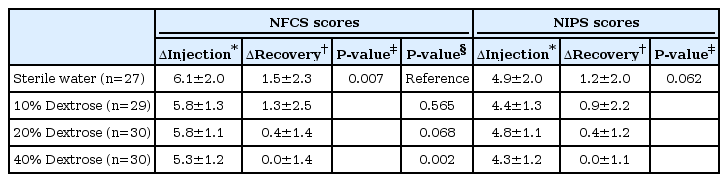
Comparison of Change in Score from Baseline to Injection and from Baseline to Recovery According to the NFCS and NIPS
DISCUSSION
This study showed that the administration of 40% dextrose prior to hepatitis B vaccination effectively relieved pain compared to sterile water on the NFCS and PIPP scales without any hyperglycemic events. However, the 10% and 20% dextrose solutions had no significant analgesic effect on the neonatal pain scores.
Although the precise mechanism has not yet been determined, sweet taste is thought to have an analgesic effect by stimulating oro-gustatory receptors and release of endogenous opioids [15,16]. A previous study showed that sweet taste is important to pain relief regardless of the carbohydrate content [17]. Sucrose water is commonly used to reduce minor procedural pain in newborns; glucose has an equivalent analgesic effect [11,18,19]. Glucose solution is easily available in the neonatal intensive care unit, whereas a sucrose solution must be prepared by the pharmacy or the nutrition team in advance because it is not commercially available in Korea. Accordingly, glucose can be used as an alternative to sucrose for providing analgesia in newborns.
Several previous randomized clinical trials have shown that a ≥20% glucose solution provides effective pain relief in newborns [20-25]. A recent meta-analysis suggested that 20% to 30% glucose has an analgesic effect [11]. However, in our study, a dextrose concentration of 20% or less did not demonstrate an analgesic effect; only the 40% dextrose solution revealed a statistically significant analgesic effect compared to sterile water.
Although 10% and 20% dextrose solutions were ineffective in reducing pain compared to sterile water, there was a positive relationship between the dextrose concentration and analgesic effect in our study. Thus, we believe that a concentration of 21% to 40% dextrose might be the cut-off range for the control of neonatal pain. In contrast, an earlier study reported that the analgesic effect plateaued off at a concentration of 25%, based on the finding that both 25% and 50% glucose showed similar effect [20]. Blass and Shah [16] and Blass and Shide [26] also suggested that a sweet solution had a flat dose-response relationship. We did not study a dextrose concentration between 20% to 40%. Dextrose concentrations between 20% to 40%. need to be included in further studies to assess the dose-response relationship and determine the exact cut-off range. The onset and duration of pain control with dextrose were not determined. Blass and Shah [16] concluded that the level of endogenous opioids peaked 2 minutes after feeling the sensation of sweetness and lasted for 5 to 10 minutes. An earlier study showed that this effect peaked at 2 minutes after injection when there was a 2-minute interval between glucose administration and a painful procedure [27]. Based on these studies, glucose was given orally 2 minutes before injection and pain scoring was done 2 minutes after the injection in our study. However, we believe that further studies are needed to investigate the ideal timing of glucose administration.
We used three pain scales — NFCS, NIPS, and PIPP — for this study. They have been used as reliable tools for assessment of procedural pain in previous studies [5,6,11]. NFCS includes multiple indicators of facial expression in neonates and NIPS assesses facial expression, cry, breathing patterns, movements of arms and legs, and the state of arousal. PIPP is available for both preand full-term infants adjusted for gestational age. Objective indicators such as heart rate and oxygen saturation were used to assess the physiologic responses [14]. Score of ≥3/8 in the NFCS [12], ≥4/7 in the NIPS [13], and ≥7/18–21 (according to the gestational age) in the PIPP scales [14] are considered to indicate pain. Based on our results, the odds ratio for pain decreased significantly with increasing concentration of dextrose, as assessed by all three pain scales based on these cut-off values. However, we finally chose the repeated measures multivariate analysis of variance as we felt that this method was more relevant for this study.
This study has several limitations. First, as it was not possible to analyze the effect of various concentrations of dextrose, we could not find a more precise, narrower range than the 20% to 30% concentration of dextrose previously reported to be effective for analgesia. We found that 20% dextrose, which was effective in a previous study, was not an effective analgesic in this study. Second, the pain scoring system we used may be of limited utility. It is essential to assess pain accurately to analyze analgesic effect. The pain scales used in this study included subjective parameters and had fundamental limitations despite being commonly used. Although the ICC between the two researchers was good, they had difficulty scoring participants in exactly the same way.
However, this study also has several strengths. First, it was a prospective, randomized, controlled, blinded clinical trial. Second, the intensity of pain was assessed by three different pain scales; we could confirm similarities in assessment with the use of these scales. Third, to our knowledge, this is the first study to evaluate the analgesic effects of various concentrations of glucose using pain scales. Fourth, we video-recorded the procedure to ensure blinding of pain scoring.
In conclusion, 40% dextrose effectively relieved minor procedural pain in newborns without causing hyperglycemic events. There was no significant analgesic effect of 10% or 20% dextrose on the neonatal pain scores. Further studies are needed to determine the lowest concentration of dextrose between 21% to 40% that is most effective and has fewer complications. There is no well-structured protocol for neonatal pain control in Korea so far, and more studies are needed to develop guidelines based on accurate understanding and evidence.
Notes
No potential conflict of interest relevant to this article was reported.